History: status post trauma with severe blood loss.
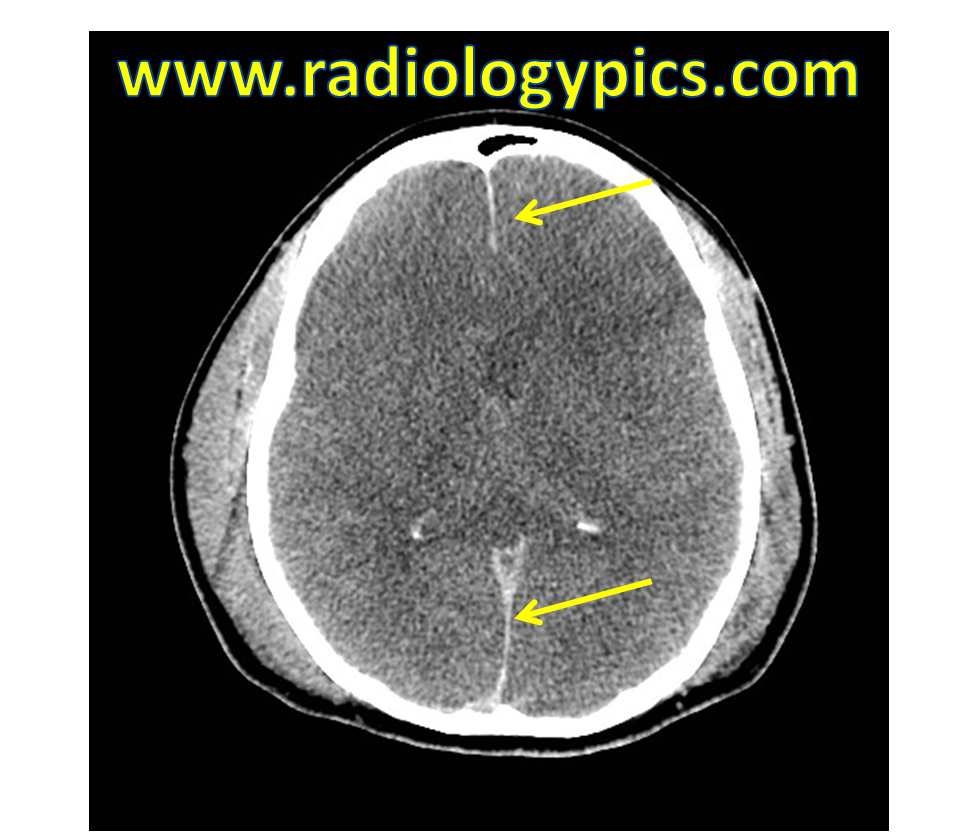
This is a case of diffuse cerebral edema secondary to exsanguination. The pathophysiology of diffuse cerebral edema in the case of exsanguination involves global brain ischemia secondary to hypoperfusion from hypovolemic shock. Brain ischemia leads to anaerobic metabolism that produces less adenosine triphosphate (ATP) and more lactate. This leads to increased release of glutamate, triggering the cytotoxic edema. Cytotoxic edema results from failure of the sodium/potassium (Na/K) pump to continue pumping sodium out of the cells and into the extracellular space. Cytotoxic edema appears as diffuse hypoattenuation of the brain parenchyma and effacement of the sulci, as seen above. The prognosis at this point is extremely poor.
The falx in the image above (yellow arrows) appears falsely hyperattenuating, which may mislead one to believe there is subdural or subarachnoid hemorrhage. Read about pseudo-hemorrhage here.




Leave a reply to Vishnu Cancel reply